Isolated Hydatid Cyst of Intestine
<p style="text-align: justify;">Hydatid cyst is zoonotic diseases mainly affect liver. Hydatid cyst involving other organ is very rare. Hydatid cyst involving other abdominal organ is mostly due to dissemination or rupture. Isolated involvement other organ is mostly due to portal venous system bypass or development of collateral in portal venous system. Primary involvement of intestine is very rare compared with other organ involvement. This is a case report of isolated involvement of hydatid cyst of large intestine.</p>
Introduction
The incidence of hydatid cyst high in liver (66%) followed by lungs (25%). Other organ involvement is quite rare. Other organ like spleen, brain, muscle, kidney, adrenal glands, bone, heart, pancreas, mesentery and intestine [1]. Hydatid cyst of intestine divided into primary and secondary. Primary hydatid cyst of intestine is very rare compared to secondary hydatid cyst. Primary hydatid cyst of intestine occurs only when Echinococcus bypass portal venous system and inoculated into the intestine. Secondary hydatid cyst occurs when intestine hydatid cyst occurs along with liver hydatid cyst or as a complication of liver hydatid cyst like rupture or dissemination [2]. Hepatic hydatid cyst mostly asymptomatic, sometimes it can present with vague abdominal pain. Intestinal hydatid cyst mostly presents with abdominal pain or intestinal obstruction.
A 34-year-old male presented with chronic abdominal pain for 3 years duration. No history of nausea or vomiting. No history of altered bowel habits like constipation, diarrhoea and bleeding per rectum. No history of loss of appetite or loss of weight. No history of any other medical co morbidities. No history of previous surgery. On abdominal examination showed diffuse lower abdominal tenderness and an ill defined mass present over the right upper abdomen. Routine blood investigations were normal. IgG antibody and ELISA serology was negative. X-ray abdomen showed calcification on right upper abdomen. Contrast computed tomography abdomen showed a well defined round laminated calcified mass of 3.2X 2.7cm seen in hepatic flexure (Figures 1& 2).
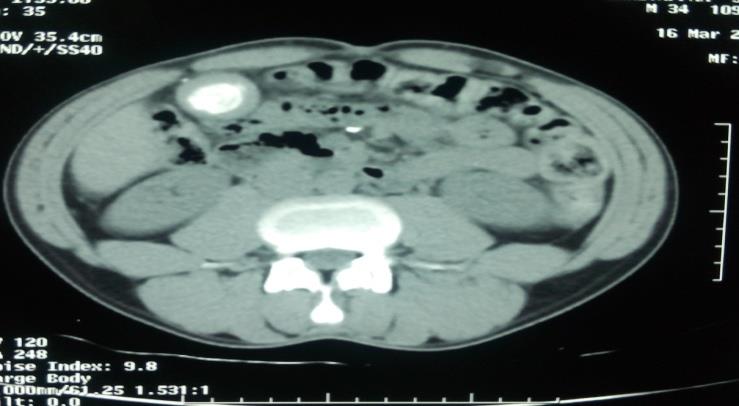




Figure 5: Histopathology showed laminated membrane beneath germinal layer. Patient diagnosed as primary hydatid cyst of intestine and underwent laparotomy and excision of affected segment of intestine (Figures 3 & 4), post operative period is uneventful. Histopathological examination confirmed features of hydatid cyst of intestine (Figure 5). Patient on post operative prophylaxis for 3 months on albendazole. No recurrence noted during follow-up.
Discussion
Hydatid cyst is an endemic disease caused by Echinococcus granulosus, Echinococcus multilocularies and Echinococcus vogeli. Large intestine is very unusual site for primary involvement of hydatid cyst [3]. Mechanism of involvement of primary hydatid cyst of liver is unclear. But there are two hypothesis suggested possible way of involvement of primary hydatid cyst of intestine. One is dissemination via lymphatic or systemic circulation or portal vein bypass by Echinococcus [4]. Most of the hydatid cyst of intestine is asymptomatic, but few cases presented with abdominal pain, mass abdomen, cyst in the stool (hydatidiarrhea), chronic intestinal obstruction and anaphylactic shock in case of rupture [4]. Most of the hydatid cyst is diagnosed usually combination of laboratory and radiological investigations. USG mostly used to screen for suspected hydatid cyst of liver. Ct is most specific and sensitive investigations for hydatid cyst. CT scan able to differentiate other cystic lesions like mesenteric cyst, pseudocyst, lymphangioma, ovarian cyst, gastrointestinal duplication cyst and congenital cyst from hydatid cyst [5]. Laboratory investigation like ELISA, IHA (Indirect haemagglutination test). Latex agglutination test and immunoblot is used to diagnose hydatid cyst [6]. False negative serological test occur mainly in size less than 9 cm, solitary cyst, extra hepatic cyst, unilocular cyst and degenerative and calcified cyst. The sensitivity of complement fixation test is 65% whereas IHA and ELISA is 85% [7]. Treatment of hepatic hydatid cyst is variable staring from medical management for disseminated or extremely morbid patient. Minimally invasive procedure like PAIR and laparoscopic management. Open surgery is rarely performed for hepatic hydatid cyst. Management of intestinal hydatid cyst mostly surgical either pen or laparoscopic depends on patient condition, location of cyst etc [8]. Complication of hydatid cyst of intestine includes hydatid peritonitis due to rupture of cyst, anaphylactic reaction, infection of the cyst, compression of adjacent organ and intestinal obstruction [9].
Conclusion
Primary hydatid cyst of intestine is one of the differential diagnoses of mass abdomen. Most of the cases asymptomatic for longer duration and it may present with abdominal pain or mass abdomen, laminated calcification mostly suggestive of hydatid cyst. Symptomatic hydatid cyst of intestine should be resected because any time it can produce complication like rupture, dissemination, anaphylaxis or intestinal obstruction.
References
-
Daldoul S, Moussi A, Zaouche A (2013) Spontaneous fistulization of hepatic hydatid cyst into the duodenum: an exceptional complication. J Coll Physicians Surg Pak 23(6): 424-426.
-
Belli S, Akbulut S, Erbay G, Koçer NE (2014) Spontaneous giant splenic hydatid cyst rupture causing fatal anaphylactic shock: a case report and brief literature review. Turk J Gastroenterol 25(1): 88-91.
-
Jenkins DJ, Lievaart JJ, Boufana B, Lett WS, Bradshaw H, et al. (2014) Echinococcus granulosus and other intestinal helminths: current status of prevalence and management in rural dogs of eastern Australia. Aust Vet J 92(8): 292-298.
-
Najih M, Chabni A, Attoulou G, Yamoul R, Yakka M, et al. (2012) Isolated primary hydatid cyst of small intestinal mesentery: an exceptional location of hydatid disease. Pan Afr Med J 13: 17.
-
Dalal U, Dalal AK, Singal R, Naredi B, Gupta S (2011) Primary hydatid cyst masquerading as pseudocyst of the pancreas with concomitant small gut obstruction- -an unusual presentation. Kaohsiung J Med Sci 27(1): 32-35.
-
Mujtaba SS, Faridi N, Haroon S (2013) Primary hydatid cyst of the neck. J Coll Physicians Surg Pak 23(10): 811-812.
-
Ayadi-Kaddour A, Mlika M, Yahyaoui M, El Mezni F (2008) Intestinal hydatidosis: uncommon location of hydatid cysts. Surg Infect 9(5): 541-543.
-
Gomez I Gavara C, López-Andújar R, Belda Ibáñez T, Ramia Ángel JM, Moya Herraiz Á, et al. (2015) Review of the treatment of liver hydatid cysts. World J Gastroenterol 21(1): 124-131.
-
Pandiaraja J (2016) Diagnostic difficulty of liver lesion. J Fam Med Prim Care 5(3): 722-724.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey